Disclaimer
The information that follows is not meant as an official account of all the dangers of high altitude climbing, nor has it been prepared by a licensed medical professional. Mountaineering is an extremely high-risk activity and should only be attempted by seasoned professionals. Please consult your physician before attempting any activity at high altitude.
I originally wrote this as a research paper in Fall 2002 for a Physiological Psychology course in college, and thought that some might find it useful here on SP. The original online issue of this Article can be found
here.
"Why do people get sick at high altitude?"
There are a variety of factors that contribute to the human body's weakness at high altitudes. Our bodies were not created to handle the incredibly frigid temperatures, the high winds, or the lack of oxygen that are common in places such as these, and thus we are forced to come properly prepared mentally and physically. It goes without saying, that ambient air temperature decreases with height, meaning that you will be much colder on the summit of an 8000-meter peak than you would when sitting on the beach in Miami. Recent developments from specialized clothing manufacturers have alleviated much of the danger posed by the temperatures and winds, though oxygen concentration is a different animal altogether.
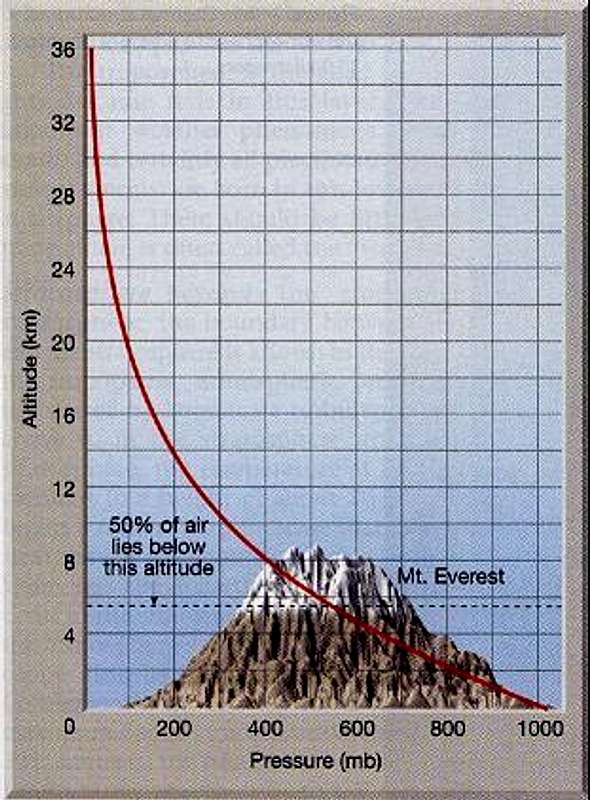
One common myth is that it is a decrease in the amount of oxygen that acts as the driver for all types of altitude sickness. The true cause, however, is the lack of atmospheric pressure. Pressure is defined as the weight exerted on the surface of the Earth by a column of air rising vertically to the very top of the atmosphere. Since mountains rise so much higher than land close to sea-level, the columns of air over them are much shorter, and thus, there is much less weight (pressure) over that part of the surface. Because of this, the air molecules are much more dispersed, so there is actually much less atmosphere up here (contributing to the significant risk of sunburn), not just less oxygen! Sea-level pressure, measured in millibars, usually tends to be around 1013mb, with some small variations based on weather phenomena. Vertical changes, however, produce huge changes in pressure (see Figure 1). In fact, when standing on the summit of Chomolungma (Mt. Everest), there is somewhere around 300-350mb which aslo varies based on the seasons (lower in winter). When you hear people say, "There is on 1/3 of the oxygen on Everest as there is at sea-level," the truth is that that the pressure has decreased to only about 30% of that by the oceans. There is actually the same concentration of oxygen in the atmosphere regardless of elevation. While this admittedly seems like splitting hairs, it is important to realize that the reduced pressure does not allow as much air into your lungs, which can therefore not absorb as much oxygen as your body needs. The way the human body reacts to this problem is what causes AMS, HACE and HAPE.
"What is the proper way to acclimatize?"
The human body is able to exist within an amazing range of environments, however, the necessary habituation processes usually take time. When climbing, it is advisable to adopt the "climb high, sleep low" strategy. Especially in expedition-style climbs, mountaineers will often climb as high as they safely can during the day, but return to a much lower elevation to sleep. Increasing the sleeping elevation by only 350m (1,150ft) per day, greatly reduces the chances of getting one the the potentially deadly altitude-related conditions (AMS, HACE & HAPE). Every 1000m (3,280ft), climbers should factor in a rest day, in order to fully get used to the new atmospheric pressure. If any member of your party doesn't feel well sleeping at a particular altitude, wait until normal functions have returned before attempting to go higher. By conservatively observing these practices, you should stay relatively safe regarding altitude-related illness.
Alpine-style climbs, on the other hand, usually entail light and fast climbing, which doesn't leave much time to "climb high, sleep low." In this situation, a specific acclimatization climb may be in order, where a group climbs a slightly lower peak observing proper acclimatization principles, and then quickly travels to their chosen mountain where they can safely complete an alpine-style ascent. Acclimatization is rapidly lost after leaving high altitudes, so fast travel and rapid re-ascent are imperative to maintaining altitude adaptation.
It should also be noted that in the "Death Zone," above 7500m (24,600ft), acclimatization is virtually impossible. There are a very few people with the genetic predisposition to be able to exist at these extreme elevations. Climbers like Ed Viesturs and the late Babu Chiri Sherpa possess a better-than-average ability to absorb oxygen into their bloodstream. While modern medicine cannot do anything to boost this ability for those of us who "didn't choose their parents well," doctors can test this genetic ability to predict who may perform well at altitude. Most people should limit their exposure to altitudes such as these to the minimum amount possible, as the human body is slowly going through the process of dying. The idea is to get up and back down fast enough such that you don't have a chance to die all the way. Viesturs describes being in the "Death Zone" as "climbing on borrowed time." If you are not extremely careful, your time may run out.
Frostbite
Although much has been done to create products that keep climbers warm in any situation, there are still areas on the planet, such as Denali, the Antarctic, and the Himalayas, that defy any attempt to tame them. Any time that the temperature is below -4°C (25°F), skin's freezing point, humans are at risk of frostbite. Since wind greatly exacerbates this effect, windproof clothes as well as thermal protection are of vital importance when climbing. The following information has been taken from
WebMD.com:
"There are three degrees of frostbite: frostnip, superficial frostbite, and deep frostbite. Although children, older people, and those with circulatory problems are at greater risk for frostbite, most cases occur in adults between 30 and 49."
"If you have frostbite, you may not realize at first that anything is wrong because the affected area will be numb. With prompt medical attention, most people recover fully from frostbite. However, in severe frostbite, permanent damage is possible, depending on how long and how deeply the tissue is frozen. In severe cases, blood flow to the area may stop and blood vessels, muscles, nerves, tendons, and bones may be permanently affected. If the frozen tissue dies, the area may need to be amputated."
For more information, see WebMD.com's full frostbite description
here.
Acute Mountain Sickness (AMS)
When traveling above 2500m (8,200ft), the effects of altitude may begin to take their toll on the human body. As the body notices that it is receiving less and less oxygen, it attempts to habituate by increasing the amount of blood flow to the brain. If it overcompensates, however, and there is too much blood flow to the brain, a process begins causing the brain to swell. The progression of this problem can result in several symptoms:
- Headache
- Exhaustion
- Shortness of breath
- Nausea or vomiting
As with any altitude-related problem the best treatment is immediate descent. Since aerobic fitness seems to have little correlation to AMS, proper acclimatization should alleviate most problems with AMS in the majority of people. As always, your doctor can provide you with much more information regarding this disorder.
High Altitude Cerebral Edema (HACE)
If the previously mentioned brain swelling progresses to higher levels, an incredibly dangerous condition, known as high altitude cerebral edema (HACE), can ensue. This problem usually does not happen below 3050m (10,000ft), and similarly to AMS, can be prevented through proper acclimatization processes. Symptoms of HACE include:
- Profoundly inhibited mental function
- Hallucinations
- Loss of muscle coordination
- Impaired speech
- Severe headache
- Nausea or vomiting
- Coma
This deadly condition can only be treated by immediate, rapid descent or by the use of a hyperbaric oxygen chamber. Your doctor can perform test on you to see how well your particular physiology responds to hypoxic conditions (lack of oxygen), so this would be advisable before any trips to the mountains. If you or anyone exhibit any signs of HACE at anytime, the best idea is to play it safe and descend to a much lower altitude. The mountains will be there next year, so make sure you will too.
High Altitude Pulmonary Edema (HAPE)
This conditions is one of the biggest killers when people venture into the higher altitudes. Another method that the body uses in attempts to get more oxygen, is to divert more bloodflow to the lungs. As with the brain, fluid build-up is at the root of the problem, and as a result can cause flu-like symptoms that will progress to death if left unattended. Climbers and others traveling to high altitudes should be watching for this condition anywhere above 2500m (8,200ft).
- Extreme difficulty breathing
- Very rapid breating rate
- Exhaustion
- Lack of motivation
- Pale complexion
- Constant coughing
- Gurgling sounds coming from chest
Not to sound like a broken record, but acclimatization is again key in preventing HAPE. Always be sure to include enough rest time, as over-exertion multiplies the likelihood that this condition will strike. After the onset of symptoms, death can ensue extremely rapidly, so immediate descent is vital.
"What does current research say about hypoxia?"
WARNING! BIO-BABBLE AHEAD!
Biologists and neuropsychologists are currently working to better understand what makes our frail bodies respond the way they do to the hypoxia (lack of oxygen) at extreme altitudes. The hope is that medications can be developed to alleviate the problematic processes such that high-altitude mountaineering will become much safer. While some may debate on whether or not this takes the adventure out of the sport, it is safe to say that most people would like to have such a medication readily available if they are rendered ill and immobile at 8000m or above.
The majority of hypoxia research up to now has concentrated on the synaptic effects of the neurotransmitter glutamate. While the short-term consequences of this condition are relatively well-documented, the long-term effects of prolonged exposure to hypoxic conditions are virtually unknown. As far as the general results of an oxygen shortage, one source notes:
"Neurons of the brain rarely regenerate, so each dead neuron is one less we have for thinking. One of the fascinating ironies of neuronal life and death is tha glutamate, the most essential neurotransmitter in the brain, is also one of the biggest killers of neurons. A large percentage of the brain's synapses release glutamate, and it is stored in large quantities. Even the cytosol of nonglutamatergic neurons has a very high glutamate concentration, greater than 3mM. An ominous observation is that when you apply this same amount of glutamate to the outside of neurons, they die within minutes."
"The voracious metabolic rate of the brain demands a continuous supply of oxygen and glucose. If blood flow ceases, as in cardiac arrest, neural activity will stop within seconds, and permanent damage will result within a few minutes. Disease states such as cardiac arrest, stroke, brain trauma, seizures, and oxygen deficiency [hypoxia] can initiate a vicious cycle of glutamate release. Whenever neurons cannot generate enough ATP to keep their ion pumps working hard, membranes depolarize and Ca2+ leaks into cells. The entry of Ca²+ triggers the synaptic release of glutamate. Glutamate further depolarizes neurons, which further raises intracellular Ca²+ and causes still more glutamate to be released. At this point, there may even be a reversal of the glutamate transporter, further contributing to the cellular leakage of glutamate."
"When glutamate reaches high concentrations, it kills neurons by overexciting them, a process called excitotoxicity. Glutamate simply activates its several types of receptore, which allow excessive amounts of Na+, K+ and Ca²+ to flow across the membrane. The NMDA subtype of the glutamate-gated channels is a critical player in excitotoxicity because it is the main route for Ca²+ entry. Neuron damage or death occurs because of swelling resulting from water uptake and stimulation by Ca²+ intracellular enzymes that degrade proteins, lipids, and nucleic acids. Neurons literally digest themselves."
"Excitotoxicity has recently been implicated in several progressive neurodegenerative human diseases, such as amyotrophic lateral sclerosis (ALS, also know as Lou Gehrig's disease), in which spinal motor neurons slowly die, and Alzheimer's disease, in which brain neurons slowly die. The effects of various environmental toxins mimic aspects of these diseases. Eating large quantities of a certain type of chickpea can cause lathyrism, a degeneration of motor neurons. The pea contains an excitotoxin called ß-oxalylaminoalanine, which activates glutamate receptors. A toxin called domoic acid, found in contaminated mussels, is also a glutamate receptor agonist. Ingesting small amounts of domoic acid causes seizures and brain damage. And another plant excitotoxin, ß-methylaminoalanine, may cause a hideous condition that combines symptoms of ALS, Alzheimer's disease and Parkinson's disease in individual patients on the island of Guam."
"As researchers sort out the tangled web of excitotoxins, receptors, enzymes and neurological disease, new strategies for treatment will emerge. Already, glutamate receptor antagonists that can obstruct the excitotoxic cascades and minimize neuronal suicide show clinical promise. Genetic manipulations may eventually thwart neurodegenerative conditions in susceptible people."
Bear, Mark F., et al. Neuroscience: Exploring the brain. Ed. 2, Lippincott Williams & Wilkins, Baltimore, MD. 2001. p.152.
Some recent studies have focused on specific brain areas in order to better explain the potential functional side-effects of hypoxia. One area of interest is the hypothalamus. One experiment published in November of 2000 noted that:
"After rats were exposed to altitude hypoxia, contents of glutamate (Glu) and asparate (Asp) in [the] hypothalamus and prepro-somatostatin mRNA (PPS-mRNA) expression in [the] periventricular nucleus, paraventricular nucleus and arcuate nucleus were increased significantly. Ketamine, a NMDA receptor antagonist, could decrease the number of PPS-mRNA neurons in rat hypothalamus evoked by altitude hypoxia, but had no effect on Glu and Asp contents evoked by altitude hypoxia. It is suggested that somatostatin may participate in [the] altitude hypoxia reaction, [since] Glu can enhance PPS-mRNA expression through [the] NMDA receptor."
Ruan, H.Z., et al. Excitatory amino acids enhance prepro-somatostatin mRNA expression induced by altitude hypoxia in the rat hypothalamus. Chinese Journal of Applied Physiology, 2000 Nov; 16 (4) pp.302-4.
Other areas of research are examining possible ways to prevent the effects of hypoxia from ever taking place and thus preventing any adverse effects. A relevant study completed and published in October 2002 explains:
"We showed recently that imidazolines exert neuroprotection against hypoxia toxicity in cerebellar and striatal neuronal cultures, through a voltage-dependent blockade of glutamatergic NMDA receptors. Here, we report that in striatal neuronal cultures from mouse embryos the imidazoline compound, antazoline, inhibits voltage-gated Ca²+ channels by acting at a phencycli-dine-like site. This effect was fast, fully reversible, voltage-dependent and predominant on P/Q- and N-type Ca²+ channels. Taken together, these results suggest that imidazolines may elicit neuroprotective effects also by decreasing the release of glutamate through inhibition of presynaptic Ca²+ channels."
Milhaud D., et al. Inhibition of voltage-gated Ca²+ channels by antazoline. Neuroreport, 2002 Oct 7; 13 (14), pp.1711-4.
Regardless of how well we currently understand the causes and effects of hypoxia, the future will definitely hold much in the way of discovery. Perhaps humans can one day venture up to the highest places on our planet without fear of adverse biological consequences. If this does come about, then climbers will have a significant choice to make: 1) climb with these medications, and eliminate the risk of high altitude-related conditions, or 2) climb without them and still maintain a sense of personal adventure. Many climbers purposefully do not use bottled oxygen, so that they do not bring the mountains down to their level; in order for a climber to truly know him or herself, he or she must discover what they can accomplish on the mountain's terms. That is not to say, however, that a little insurance wouldn't be appreciated, just in case.















 I just wanted to give my 2 cents on frostbite. I grew up in a cold climate, and winter is my favorite time of year. Any excuse to get out and have fun in the snow I take. All these years, up until last week, I had only had frostbite once, and that was on my wrist where my gloves ended and my coat sleeve began. So I was very surprised last week when after a day of skiing at Brighton, Utah (not exactly a cold place -- the temperature was around -8C [17 F]) I ended up with frostbitten cheeks. It's weird cause I was dressed the same as usual and I would occasionally warm my face with my hand while on the lift. It was really windy so maybe the wind chill was the factor, and also I put on sun block thinking it might form a protective layer, but in retrospect the sun block might have contributed to the problem by keep moisture in which ended up freezing, or maybe the sun block itself froze leaving a thin ice layer on my cheeks. The point is Jack Frost is out there ready to nip you, so don't take any chances and cover up!
I just wanted to give my 2 cents on frostbite. I grew up in a cold climate, and winter is my favorite time of year. Any excuse to get out and have fun in the snow I take. All these years, up until last week, I had only had frostbite once, and that was on my wrist where my gloves ended and my coat sleeve began. So I was very surprised last week when after a day of skiing at Brighton, Utah (not exactly a cold place -- the temperature was around -8C [17 F]) I ended up with frostbitten cheeks. It's weird cause I was dressed the same as usual and I would occasionally warm my face with my hand while on the lift. It was really windy so maybe the wind chill was the factor, and also I put on sun block thinking it might form a protective layer, but in retrospect the sun block might have contributed to the problem by keep moisture in which ended up freezing, or maybe the sun block itself froze leaving a thin ice layer on my cheeks. The point is Jack Frost is out there ready to nip you, so don't take any chances and cover up!
Comments
Post a Comment